— Long-ignored patches of progressively hardening skin finally receive a rare diagnosis
by
Kate Kneisel, Contributing Writer, MedPage Today
February 5, 2024
Why did this 11-year-old boy begin to experience increasingly limited range of motion in his right leg, years after developing progressive skin problems on the same limb?
The boy had no previous medical conditions and his parents were also both healthy. However, for the past 7 years, the boy had been affected by patches of increasingly hardened skin on his right thigh and buttock, reported Jiu-Hong Li, MD, PhD, of the First Hospital of China Medical University in Shenyang, and colleagues in JAMA Dermatology.
Physical examination revealed a poorly defined, stony-hard plaque on his right thigh that extended from above his knee cap to his right buttock. The affected skin had little elasticity, was hyperpigmented, and had mildly excessive hair growth.
Results of routine blood and lab tests for autoantibodies, immunoglobulins, C-reactive protein, and erythrocyte sedimentation rate all returned normal. The team ordered an MRI of the patient’s right thigh, which revealed slight thickening of subcutaneous tissue and T2 signal abnormality.
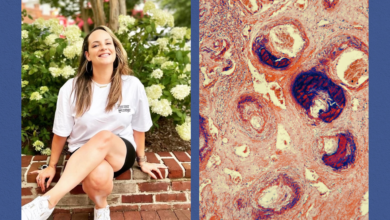
Clinicians biopsied the affected skin on his right thigh; the sample was sent for histopathological examination and alcian blue staining.
“Histopathological examination revealed normal epidermis and a mild pigmentation along the basal layer with a subtle increase in density of fibroblasts extending to the subcutis and forming adipocyte entrapment but no evidence of inflammation,” Li and co-authors noted. “There was dense reticular dermis extended below well-preserved appendages.”
Immunohistochemical staining indicated an increased expression of CD34 in the reticular dermis, while findings of the alcian blue staining were negative.
The team arrived at a diagnosis of segmental stiff skin syndrome (SSS) based on the clinical morphology, histological features, and MRI findings. Clinicians recommended physical therapy to prevent joint contracture.
Discussion
SSS is a rare condition of the cutaneous connective tissue; it is marked by stony-hard skin, mild hypertrichosis, and hyperpigmentation, Li and co-authors explained. The disorder often affects the buttocks and thighs, and other areas with rich fascia. Beyond its dermatologic effects, SSS is often associated with abnormal gait and posture and joint contractures, and may affect movement of the chest and abdomen.
Why and how SSS develops is poorly understood, the authors noted. However, they cited recent reports that suggested that it “may be associated with primary fibroblast disorder, primary fascial dystrophy, or heterozygous mutations in the FBN1 gene.”
This clinically distinct variant of SSS is characterized by the same histopathologic features as generalized SSS, they pointed out, including “thickening and compactness of collagen fibers in dermis with entrapped adipocytes, no infiltration of inflammatory cells, no atrophy of adnexa, and thickening of fascia.”
“Segmental SSS has the characteristics of unilateral predominance, later onset, and lack of evolution into a generalized disease,” they added.
Because presentation of segmental SSS is rare or atypical, clinicians should consider differential diagnoses including linear morphea, linear connective tissue nevi, and eosinophilic fasciitis.
Linear morphea, a variant of localized scleroderma, causes “unilateral skin tightness and induration in a linear distribution following the Blaschko lines,” the authors wrote. It generally has a later onset, and presents with more localized and asymmetric skin changes. “Pathologically, linear morphea is characterized by homogenization of collagen bundles in the dermis and subcutis associated with lymphoplasmacytic infiltration and perivascular inflammation,” they noted.
Eosinophilic fasciitis is a variant of scleroderma that affects the distal limbs, rapidly causing symmetrical areas of tender swelling that gradually develop into hard plate-like plaques. Its dermatologic symptoms may be accompanied by peripheral eosinophilia and systemic symptoms, including fever, weight loss, fatigue, and weakness or lack of energy. Eosinophilic fasciitis may emerge after very strenuous physical exercise.
The third diagnosis to eliminate is linear connective tissue nevi, a painless, hamartomatous lesion that tends to develop on the trunk and limbs in early childhood. It is characterized by normal skin color or hypochromic plaques or nodules that develop slowly in linear arrangements. Lab tests tend to show “an irregular increase of collagen fibers in the dermis without fibroblastic proliferation,” the authors wrote.
“Early recognition of segmental SSS may help prevent joint contracture and avoid inappropriate medical treatment,” Li and co-authors concluded. There are few treatment options for the condition, and results tend to be unsatisfactory. Because of their antifibrotic effects, treatment with losartan and mycophenolate mofetil may result in some improvement in some patients.
As Li and colleagues recommended for this patient, undertaking rehabilitation exercises early in the disease course may help patients avoid joint restriction and preserve mobility. In addition, according to a recent study, supplementary treatment with secukinumab (Cosentyx) may help reduce skin stiffness and improve range of motion.
-
![author['full_name']](https://clf1.medpagetoday.com/media/images/author/KKneisel_188.jpg)
Kate Kneisel is a freelance medical journalist based in Belleville, Ontario.
Disclosures
Yang and co-authors reported no conflicts of interest.
Primary Source
JAMA Dermatology
Source Reference: Yang Y, et al “Segmental skin induration in a boy” JAMA Dermatol 2024; DOI: 10.1001/jamadermatol.2023.4235.